
From the 1Department of Palliative Care, Policy and Rehabilitation, Cicely Saunders Institute, Florence Nightingale Faculty of Nursing, Midwifery and Palliative Care, King’s College London, 2Regional Hyper-acute Rehabilitation Unit, Northwick Park Hospital, London, UK, 3Centro de Medicina de Reabilitaçãode Alcoitão, Serviço de Reabilitação de adultos 3, Estoril, Portugal, 4Neurorehabilitation, Gailtal-Klinik, Hermagor, Austria, 5Department of Neurology, University of California, Davis, Sacramento, CA, USA, 6Department of Biometry, Ipsen Pharma, Boulogne-Billancourt, France, 7Medical Affairs, Ipsen Pharma, Cambridge, MA, USA, 8Centre for Nursing and Midwifery Research, University College London Hospital, London, UK
*ULIS-III study group. Australia: Ian Baguley, Arun Aggarwal, John Olver, John Estell, Steven Faux, Edwin Luk, Katya Kotschet, Andrew Hughes, Rachael Nunan. Austria and Germany: Bernhard Haslinger, Petra Baum, Cornelia Mobius, Urban Fietzek, Chi Wang Ip. Brazil: Tae Mo Chung, Régina Helena Chueire, Carla Heloisa Cabral Moro. France: Alexis Schnitzler, Claire Delleci, Anne-Laure Ferrapie, Marie-Eve Isner-Horobeti, Dominic Perennou. Hong Kong: Ching Man Leung. Italy: Michela Cosma, Carlo Caltagirone, Manuela Diverio, Paolo Girlanda, Giancarlo Ianeri, Marzia Millevolte, Franco Molteni. Mexico: Jorge Hernandez Franco, Juan Francisco Gomez Hernandez, Sandra Quinones Aguilar, Laura Patricia De La Lanza Andrade. Philippines: Raymond Rosales, Jeanne Flordelis. Poland: Dariusz Koziorowski, Anna Potulska, Monika Rudzinska. Portugal: Eduarda Afonso, Ana Rolo Duarte. Russia: Svetlana Khatkova, Alexey Korenko; Dina Khasanova; Dmitry Okhabov; Elena Arefyeva; Denis Karpov; Andrey Korolev. Taiwan: Yi-Chung Lee, Sen-Wei Tsai. USA: Jessica Tate, Thomas L. Davis, Cynthia Marciniak, Atul Patel.
Objective: To describe the utility of a structured approach to assessing effectiveness following injection with botulinum toxin-A alongside physical therapies, within the first cycle of the Upper Limb International Spasticity-III (ULIS-III) study.
Methods: ULIS-III (registered at clinicaltrials.gov as NCT02454803) is a large international, observational, longitudinal study of adults treated for upper-limb spasticity. It introduces novel methods for the structured evaluation of person-centred goal attainment alongside targeted standardized outcome measures: the Upper limb Spasticity Index, and the Upper Limb Spasticity Therapy Recording Schedule.
Results: A total of 953/1,004 enrolled patients (95%) completed cycle 1. Mean overall goal attainment scaling (GAS) T scores were 49.8 (95% confidence interval 49.2–50.3; 67.1% of patients met their primary goal, with highest achievement rates for goals related to involuntary movement, (75.6%) and range of movement (74.4%). Standardized measures of spasticity, pain, involuntary movements, active and passive function, all improved significantly over the treatment cycle. Overall, 59.7% of patients saw a therapist following botulinum toxin-A injection. Interventions varied, as expected, with the set treatment goals. After controlling for concomitant therapies using the upper limb spasticity therapy recording schedule, significant differences in injection intervals (p < 0.001) were seen between the commercially-available botulinum toxin-A agents.
Conclusion: The results of this study confirm the utility of the Upper Limb Spasticity Index and Upper Limb Spasticity Therapy Recording Schedule as a structured approach to capturing goal-setting, therapy inputs and outcomes assessment.
This paper presents the first results from the ULIS-III study, a large international study which explores real life clinical practice in the integrated management of upper-limb spasticity, using Botulinum Toxin-A (BoNT-A) in conjunction with physical therapies. ULIS-III is the first study to use the Upper Limb Spasticity Index (ULS Index), a system for assessing the benefits of treatment that combines recording how well the intended goals for treatment were achieved, alongside standardized measures to improve the comparability of outcomes. The data confirm good overall response rates. Importantly, when standardized measures are appropriately targeted on the individual’s priority treatment goals, they demonstrate clear measurable improvements in daily function. It is also the first study to use the Upper Limb Spasticity Therapy Recording Schedule (ULSTR) to systematically record and describe the physical therapies provided. It shows how this information helped us to explore differences between BoNT-A products in the time that each injection lasts before the next one is needed.
Key words: botulinum toxin-A; goal attainment scaling; physical therapy; post-stroke spasticity; stroke rehabilitation.
Accepted Oct 23, 2020; Epub ahead of print Nov 18, 2020
J Rehabil Med 2021; 53: jrm00133
Correspondence address: Lynne Turner-Stokes, Regional Rehabilitation Unit, Northwick Park Hospital, Watford Road, Harrow, Middlesex, HA1 3UJ, UK. E-mail: lynne.turner-stokes@doctors.org.uk
Doi: 10.2340/16501977-2770
National and international guidelines recommend botulinum toxin type A (BoNT-A) as a safe and effective focal intervention for reduction of spasticity (1–3). There is a large body of level one evidence for BoNT-A from controlled clinical studies (4–8), but these do not consider the diversity of patient presentation, nor the varied clinical approaches to treatment used in real-life clinical practice worldwide. Moreover, the wide range of individual treatment goals poses a challenge for the evaluation of outcomes. Individual patients often have very different expectations and needs from spasticity management (9), which have great impact on how treatment “success” can be defined and interpreted.
Large observational studies can improve our understanding of the complexities of how BoNT-A is used in routine clinical practice. The Upper Limb International Spasticity (ULIS) programme represents a series of large international observational studies to describe current clinical practice in the application of BoNT-A in upper limb spasticity (10–12). In line with clinical guidelines (1, 2), the programme promotes an integrated approach to spasticity management, in which BoNT-A is used in conjunction with physical therapies to optimize outcomes. The programme started in 2008 and has taken an iterative approach to study design. At each stage, we have refined our approaches to goal-setting and outcome measurement. The central theme across the programme has been the use of goal attainment scaling (GAS) as a person-centric measure that captures outcomes from management of spasticity across a diverse range of goal areas. However, key learning-points from the second stage of the programme (ULIS-II) were the need for: (i) systematic collection of data to quantify and describe concomitant therapies; and: (ii) a more structured and time-efficient approach to goal-setting recorded alongside standardized measures to improve comparability of outcomes while maintaining a patient-centred approach (12).
The ULIS-III study introduces 2 important new methods for the systematic collection of input and outcome data in the context of routine clinical practice:
ULIS-III was the first study to apply these measures. With > 1,000 patients recruited in > 50 centres, the rich dataset not only provides detailed description of real-life clinical practice, but also supports interrogation of the various treatment components in ways that were not previously possible. For example, differences in the specific biotypes and manufacturing processes of the various BoNT-A products give rise to known differences in potency (14) and may also impact on their relative duration of efficacy. However, this has not yet been tested in routine practice because comparison may be confounded by variation in the type, frequency and intensity of physical therapies. Systematic recording of the ULSTR now enables us to explore this for the first time.
The full study will assess outcomes from integrated spasticity management longitudinally over a 2-year period. This pre-specified interim analysis documents the utility of the ULS Index over the first BoNT-A injection cycle, by assessing goal attainment and treatment effectiveness on the standardized rating scales and by comparing outcomes with the earlier ULIS-II study. In addition, as ULIS-III includes treatment with any of the 3 commercially-available BoNT-A products, multivariate analysis was used to compare their duration of efficacy (as reflected by the time to re-treatment), while controlling for concomitant therapies captured by the ULSTR.
Full details of the ULIS-III methodology have been described previously (13). In brief, ULIS-III is a 2-year observational, prospective, longitudinal cohort study conducted at 57 study centres across 14 countries. The study was conducted in compliance with Guidelines for Good Pharmacoepidemiology Practices (GPP). Marketing authorization for the use of BoNT-A in this context was ensured for each participating country prior to the start of the study. Ethical approval and written informed consent to the recording of anonymous data were obtained in countries where this was required. Recruitment took place over a 2-year period between January 2015 and December 2016. The minimum sample size for enrolment was 1,000 patients, based on the primary effectiveness measure (cumulated GAS T score) and a 90% power to allow meaningful comparisons between groups across the full 2 years of the study. In order to ensure a representative sample and avoid recruitment bias, each centre recruited a maximum of 20–30 patients, either consecutively or selected in a regular pattern. The study is registered at clinicaltrials.gov (NCT02454803).
Study sample
The main inclusion criteria required patients to be consenting adults ≥ 18 years with upper-limb spasticity in whom a decision had already been made to inject BoNT-A; patients could be new to BoNT-A treatments or previously treated. This analysis includes patients who received at least one injection of BoNT-A and who underwent at least one assessment of goal attainment using the GAS (effectiveness population).
Study design
In accordance with the observational nature of this study, clinicians were free to choose targeted muscles, BoNT-A preparation, injected doses, number of points and volume for each point, and use of injection guidance (electromyography (EMG), electrical stimulation or ultrasound) or not, in accordance with their usual practice, and with their local Summary of Product Characteristics (SPC) and therapeutic guidelines. The timing of follow-up was at the discretion of the investigator, based on their usual practice and the nature of the goals set, usually between months 3 and 5. Patients participated in concomitant therapies as per usual practice, and all activities were recorded in the ULSTR, which records the number, duration and types of non-pharmacological interventions (13).
Outcomes
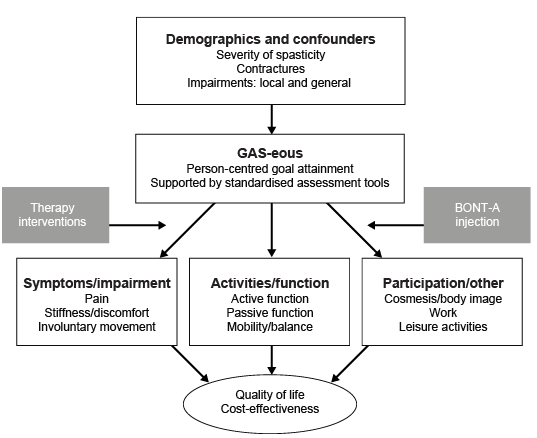
All primary and secondary goals and outcome assessment data were documented in an electronic case report form (eCRF) at each visit. As previously described, the ULS Index consists of an assessment battery with 3 main components (Fig. 1) (13):
1. Severity of presentation (demographics, distribution and severity of spasticity and any contractures) and severity of impairment (local and general) and confounding factors.
2. Goals for treatment captured using the Goal Attainment Scaling Evaluation of Outcome for Upper Limb Spasticity (GAS-eous) tool (13). This provides a structured approach to GAS, capturing the goals negotiated between patient and team (according to their individual priorities for treatment), with associated measurement parameters within 6 key goal areas (pain, involuntary movement, range of movement, passive function, active function and mobility). Goal attainment scaling is implemented using the GAS-Light method (15). In brief, goal attainment for each goal is recorded on a 5-point scale (–2 to +2) and assimilated into an overall GAS T score, using the mathematical formula described by Kiresuk & Sherman (16). If goals are set in an unbiased fashion so that they are over- and under-achieved in equal proportions, the GAS T scores should be normally distributed around a mean of 50 with a standard deviation (SD) of ±10.
3. Standardized measures are chosen from a limited set of validated tools according to the goal areas for treatment. In addition to the Modified Ashworth Scale (MAS, which is assessed in all patients), measures include:
Since this was an observational study conducted in routine clinical practice, reporting of related adverse events followed the standard regulations related to spontaneous adverse event reporting for marketed products, and is not recorded here.
Fig. 1. Upper Limb Spasticity Index (with permission from (13)). BONT-A: botulinum toxin type A; GAS-eous: Goal Attainment Scaling Evaluation of Outcome for Upper Limb Spasticity tool.
Statistical analysis
All statistical evaluations were performed using the Statistical Analysis System (SAS V.9.4; SAS Institute, Inc, Cary, NC, USA). As this was a non-interventional study reflecting real-life clinical practice, missing data were expected, and no imputations were made. The primary outcome was the GAS T score, calculated according to the method described by Kiresuk & Sherman (16). We also report descriptive statistics (n (%)) for categorical data and mean and 95% CI or median [range] for scaled data. Change from baseline for scaled data were analysed using paired t-tests, and change in FAC was analysed using the Wilcoxon signed-rank test. Patients classed as “Responders” were those who achieved their primary goal, either as expected or better than expected (GAS score 0, +1 or +2). To examine differences in the duration of efficacy between the different BoNT-A preparations while controlling for concomitant treatment, a multivariate linear model was developed to determine factors influencing the duration of the injection interval between the first and second treatment cycles. In the first step, univariate analyses were used to identify candidate covariates potentially associated with interval duration, including toxin, previously treated for upper-limb spasticity with BoNT, time from event onset to Cycle 1, distribution of spasticity, dominance of affected limb, indication of lower limb spasticity, duration of BoNT-A prior to study, systemic anti-spastic medications, injection guidance technique and mean indexed dose. All variables with a p-value < 0.20 in the univariate analyses were entered into the multivariate model selection process along with age, sex and concomitant physical therapies (type of therapists seen and number of therapy occasions), which were to be included in the multivariate model, irrespective of p-value in the univariate analysis step.
Sample description
Of the 1,004 patients enrolled, 953 met the inclusion criteria for inclusion in the effectiveness population and were included in this analysis. Patients were enrolled in Australia (n = 115, 10 sites), Austria (n = 22, 1 site), Brazil (n = 47, 3 sites), France (n = 105, 5 sites), Germany (n = 51, 5 sites), Hong Kong (n = 15, 1 site), Italy (n = 140, 7 sites), Mexico (n = 27, 4 sites), Philippines (n = 34, 2 sites), Poland (n = 59, 3 sites), Portugal (n = 73, 3 sites), Russia (n = 168, 7 sites), Taiwan (n = 25, 2 sites) and the USA (n = 72, 5 sites).
As shown in Table I, the mean (SD) age was 54.0 years (SD 15.3) and 56.3% were male. The cohort mainly comprised patients with chronic spasticity (mean time since onset 7.6 years); most commonly due to acquired brain injury (> 90%). Over 80% of patients had segmental (rather than focal) spasticity, and most (> 90%) had both proximal and distal spasticity. Between a third and half of patients had associated communication, emotional/behavioural and/or sensory impairments.
Treatment
Two-thirds of patients (n = 635; 66.6%) had received a previous injection(s) of BoNT-A in the upper limb. The median duration of BoNT-A treatment prior to study enrolment was 2.0 years [range 0.0–20.9 years]. Taken overall, the median number of muscles injected was 5 (range 1−16), with most patients receiving an injection in the forearm (92.3%), followed by upper arm (72.9%), hand and fingers (39.6%) and shoulder (39.9%) (Table I). Nearly three-quarters of the injections were given using at least one form of guidance. In this cohort, abobotulinumtoxinA (Dysport®) was the most commonly used agent (63.2% at first visit), followed by onabotulinumtoxinA (Botox®, 25.3%) and incobotulinumtoxinA (Xeomin®, 10.9%) (Table SI). Median doses per muscle are shown in Table SII. The most frequently injected muscles were the flexor digitorum superficialis, followed by the flexor carpi radialis and biceps brachii.
Table I. Baseline demographics and severity of presentation
Data regarding non-pharmacological treatment were captured by the ULSTR and was available for 818/953 patients (data missing for 135 patients). Overall, 488 patients (59.7%) received professional intervention (from a therapist and/or therapy assistant) during Treatment Cycle 1. Of these, 84.6% saw a physiotherapist (median 20 times), 36.1% saw an occupational therapist (median 13 times), 4.1% saw a therapy assistant (median 7 times) and 9.0% saw another allied professional (median 14.5 times). As shown in Table II, passive stretch and positioning were the most commonly-applied interventions across most primary goals. As expected, subtle differences were observed in the types of interventions chosen for each primary goal area. For example, interventions, such as strength training, task practice and electrical stimulation, were applied more often in patients whose primary goal related to active function, as opposed to other goal areas. However, a range of interventions is expected as most patients have goals in more than one area.
Table II. Types of non-pharmacological therapies by primary goal area
Goal attainment over one treatment cycle
The mean (SD) time between goal-setting and goal evaluation was 84.6 days (SD 96.2 days), including 57.5% of patients who only had their goal evaluation assessment at the time of next reinjection. Mean [95% CI] GAS T scores increased from 36.7 [36.5–36.9] at baseline to 49.8 [49.2–50.3] at the end of the cycle.
Overall rates of primary goal achievement were lower in Treatment Cycle 1 of ULIS-III than the earlier ULIS-II study (67.1% met their primary treatment goal during Treatment Cycle 1 vs 79.6% of patients in the ULIS-II study). As shown in Table III, goals with the highest rates of achievement were involuntary movement, (75.6%) and range of movement (74.4%). Rates of primary goal achievement were higher for goals related to passive function vs active function (72.8% vs 50.0%, respectively) (Fig. 2).
Table III. Goal attainment
Fig. 2. Rates of primary goal achievement.
Taking primary and secondary goals together, the rates of goal achievement were highest for the goal domains of range of movement (75.4% of set goals), “involuntary movements”’ (75.1%), passive function (72.1%) and pain (65.9%) and were lower for active function (48.2% of set goals). Although other goals were selected infrequently, they were generally achieved, emphasizing the need to maintain the personalized element of goal-setting, which this approach supports.
Standardized ULS Index outcomes
Within the ULS Index, standardized measures are recorded only if relevant to the chosen goal areas. As such, variable denominators were expected. The mean [95% CI] reduction in MAS-Total score was –0.5 [–0.6 to –0.4] points, which was statistically significant vs baseline (p < 0.0001). Pain scores, ARRS, ULS-NIS and ArmA scores also decreased significantly over the treatment cycle (all p < 0.0001) (Table IV). These changes were, not only statistically significant, but were also clinically important. For the 346 patients with pain primary or secondary goals; e.g., the mean reduction in pain scores was nearly 3/10 points. For those with goals related to passive and active function, the mean changes in ArmA subscales were –3.5 (passive sub-scale) and –3.2 (active sub-scale): both well in excess of the published minimum clinically-important differences of –2.5 and –1.1, respectively (22). Of the 209 patients with goals related to involuntary movements, 42% showed improvement in ARRS modal scores, while only 5% showed worsening. For the relatively small number of patients (n = 34) with goals related to mobility, there was a general shift in the Functional Ambulation Category (FAC) to greater independence (p = 0.047), although one patient worsened from Dependent Level 1 to Level 2.
Table IV. Change from Treatment Cycle 1 baseline to end of Treatment Cycle 1 in total scores of Upper Limb Spasticity Index (ULS Index) standardized measures
Time to re-injection
Of 837 patients who had a second injection cycle during the study, 783 (93.5%) received the same BoNT-A product. For this subgroup the mean injection intervals were 189.5 days with abobotulinumtoxinA (n = 485), 149.5 days with onabotulinumtoxinA (n = 164) and 147.4 days with incobotulinumtoxinA (n = 70) (Fig. 3). Univariate analyses identified BoNT-A product, BoNT-A indexed dose and previous treatment with a BoNT-A as potentially significant covariates (p < 0.2), with longer injections intervals associated with higher doses and for BoNT-naïve status. After controlling for these factors, differences between BoNT-A products in the first cycle injection intervals remained. Patients treated with abobotulinumtoxinA had, a significantly longer interval between the first and second injection than patients treated with other BoNT-A products by more than 30 days (p < 0.001).
Fig. 3. Mean time (in days) between patients’ first and second injections (injection interval, raw data). p-values were obtained from the multivariate linear model, including age, sex, concomitant physical therapies and other treatment factors (botulinum toxin type A (BoNT-A) product, BoNT-A dose and prior treatment with a BoNT-A) as covariates. aboBoNT-A: abobotulinumtoxinA, onaBoNT-A: onabotulinumtoxinA, incoBoNT-A: incobotulinumtoxinA
The ULS Index provides a novel approach to outcome measurement in the field of spasticity and this article reports its first application in real-life clinical practice from a large international cohort of patients from 14 countries spanning 4 continents. Although previous trials of BoNT-A have readily demonstrated change at the level of impairment, they have often failed to demonstrate change in function (7, 8, 23). Amongst the reasons for this were the diversity of patients and goals for treatment, and the use of broad-based measures that were insensitive to the type of changes that may be expected from focal treatment of spasticity (24). Our findings show that, when standardized measures are appropriately targeted on the intended goals for treatment, it is possible to demonstrate gains in both passive and active function that are not only highly statistically significant, but also clinically important. This method of targeting standardized measures to the intended goals for treatment is not only important for spasticity management but has wider application in other areas of clinical practice where diversity of presentation and goals for intervention limit the applicability of the same measures in all cases.
The ULIS programme has been ongoing for over a decade, and its focus on systematic evaluation of individual goal achievement has helped lead to important changes in clinical practice. Throughout the programme we have progressively refined the approach to outcome measurement. The previous arm of the programme (ULIS-II) (11, 12) used an open approach to goal-setting. Although GAS provided a sensitive measure to record attainment of the intended goals for treatment, participating teams found it quite difficult and time-consuming to apply in a busy clinic setting. The quality of goal-setting was poor; less than a quarter (24%) of centres achieved the optimal A++ quality ratings for goal-setting (11) and the overall achieved GAS T score of 52.0 suggested a tendency to set goals somewhat over-cautiously (12). The introduction of structured goal-setting using the GAS-eous tool in ULIS-III has improved the quality of goal-setting by the participating teams, with 79% of centres now achieving A++ quality ratings (13) and the overall achieved GAS T score of 49.8 is closer to 50, indicating more accurate prediction of goal achievement at baseline. Overall rates of primary goal achievement decreased from 79.6% in ULIS-II to 67.1% in ULIS-III, which is likely to reflect, at least in part, the tighter goal definition of goals using the GAS-eous tool. However, the lower proportion of primary goal achievement may also reflect the diversity of this more general neurological patient population compared with the post-stroke patient cohort included in ULIS-II. For example, more patients in ULIS-III than in ULIS-II had communication impairment (43.4% vs 34.9%) and cognitive impairment (31.6% vs 21.5%).
Our rates of goal attainment compare favourably to the BEST Study in which 33% of patients had achieved their primary active function goal and 41% had achieved their secondary (active or passive) functional goal after the first cycle of onabotulinumtoxinA (25). Also to the Australian multicentre trial published by McCrory et al. in 2010 (26), which used an unstructured approach to GAS, achieving T scores of only 35.7 after one cycle of abobotulinumtoxinA. The Early Bird study assessed goal attainment in patients treated with abobotulinumtoxinA and categorized according to time since stroke (early-start, medium-start and late-start treatment) (27). Whereas early-start patients were more likely to choose pain and active function as their primary goals, patients in the late-start group were more likely to choose goals supporting ease of care or ease of therapy. Aside from improvements in mobility and ease of therapy (significantly higher rates of achievement in the late-start vs early-start group), no significant differences in goal attainment were found, and all groups at least partially achieved their goals (27). While the TOWER study examined goal attainment following injection of incobotulinumtoxinA (28), it reported only the percentage of patients attaining 1, 2 or 3 goals and so does not provide comparable data. Such comparisons serve to highlight the continued improvements in goal-setting and integrated spasticity management made in recent years.
This study also presents the first published data from application of the ULSTR, which provides systematic prospectively-collected information on the various concomitant non-pharmacological interventions employed in conjunction with an injection of BoNT-A. Such data are vital because physical therapies form a critical component of integrated spasticity management and are expected to impact on outcome (especially in the context of goals for active function). This information can also be used to explore the contribution of separate components of treatment. In this study, data from the ULSTR supported multivariate analyses, which indicated that, after controlling for concomitant physical therapies, patients treated with abobotulinumtoxinA had a significantly longer time interval (> 30 days) between the first and second injection than patients treated with other BoNT-A products. This was true for patients who were previously treated and those who were naïve to prior BoNT-A treatment, although BoNT-A-naïve patients showed a general trend towards longer injection intervals than those previously treated for upper-limb spasticity. While randomized controlled studies are able to set consistent criteria for reinjection (29), our observational data reflects routine clinical decision-making where injectors consider other factors, such as treatment history and patient preference. Further head-to-head testing, in randomized controlled trials and longitudinally in the full ULIS-III dataset is warranted, but a possible explanation for the different durations of response could be the different amounts of active neurotoxin at the approved doses for each product (30).
As in the prior ULIS II study (12), the present study also demonstrates wide variation in clinical practice with respect to the selection of muscles and approach to injection, which may reflect individual diversity of presentation or clinician preference. Once the full longitudinal dataset is complete, it will support further exploration of what works best for which patients: the types of non-pharmacological physical treatments that are most effective following BoNT-A injections; the relationship of physical interventions applied for which types of goal; the impact of different intensities of therapy intervention and the different doses of BoNT-A required are key questions. Systematic collection of the ULS-NIS will enable us to further control for confounding factors (such as the other impairments arising from significant brain injury), which may otherwise limit the effects of intervention for spasticity.
Strengths of this study include its size and proximity to clinical practice as well as its truly global nature and the inclusion of all BoNT-A products, albeit in proportions that are not representative of general usage. However, we also recognize several limitations. Some of these are inherent to all observational studies and include the lack of a control group and the level of missing data (although the latter was less than expected). Limitations specific to this analysis include a number of sources of selection bias:
These issues and others will be explored further once the full longitudinal dataset is available, which will help us meet our key objective of understanding which patients are most likely to respond best to BoNT-A treatment. However, we believe that the ULIS-III interim first cycle data highlight that the utility of the ULS Index and ULSTR in documenting treatment effectiveness is of practical relevance to BoNT-A injectors worldwide. The findings of significant differences in the injection intervals used for the 3 commercially available products highlight important product differences that injectors should be aware of when designing a spasticity management programme that includes BoNT-A injections.
The authors thank all the investigators and patients who participated in this trial. We also thank Anita Chadha-Patel, PhD, of ACP Clinical Communications Ltd (Hertfordshire, UK) for providing medical writing support, which was funded by Ipsen (Paris, France) in accordance with Good Publication Practice guidelines. Financial support for manuscript preparation was also provided through the Northwick Park Charitable Funds.
Funding. This work was supported by Ipsen Pharma.
Conflicts of interest. LTS, KF, JJ, AB and SA all received honoraria from Ipsen for undertaking this research. LTS and SA have a specific interest in outcomes evaluation and have published extensively on the use of GAS in this context, as well as a number of the other standardized measures. All of these tools are freely available, however, and they have no personal financial interest in any of the material mentioned in this article. KF has a specific interest in outcomes evaluation and the use of the ICF in clinical settings. He has no personal financial interest in any of the material mentioned in this article. JJ has a particular interest in clinical and instrumental spasticity evaluation methods, goal-setting, treatment strategies/techniques and outcome measurement. He has no personal or financial interest in any of the material mentioned in this article. AB has a particular interest in inclusion and patient-centred care, and has no personal or financial interest in any of the material mentioned in this article. PM and AL are employees of Ipsen.
Data sharing. Ipsen will share aggregated data that underlie the results reported in this article with qualified researchers who provide a valid research question. Study documents, such as the study protocol and clinical study report, are not always available. Proposals should be submitted to DataSharing@Ipsen.com and will be assessed by a scientific review board. Data are available beginning 6 months and ending 5 years after publication; after this time, only raw data may be available.


 Click to show fullsize
Click to show fullsize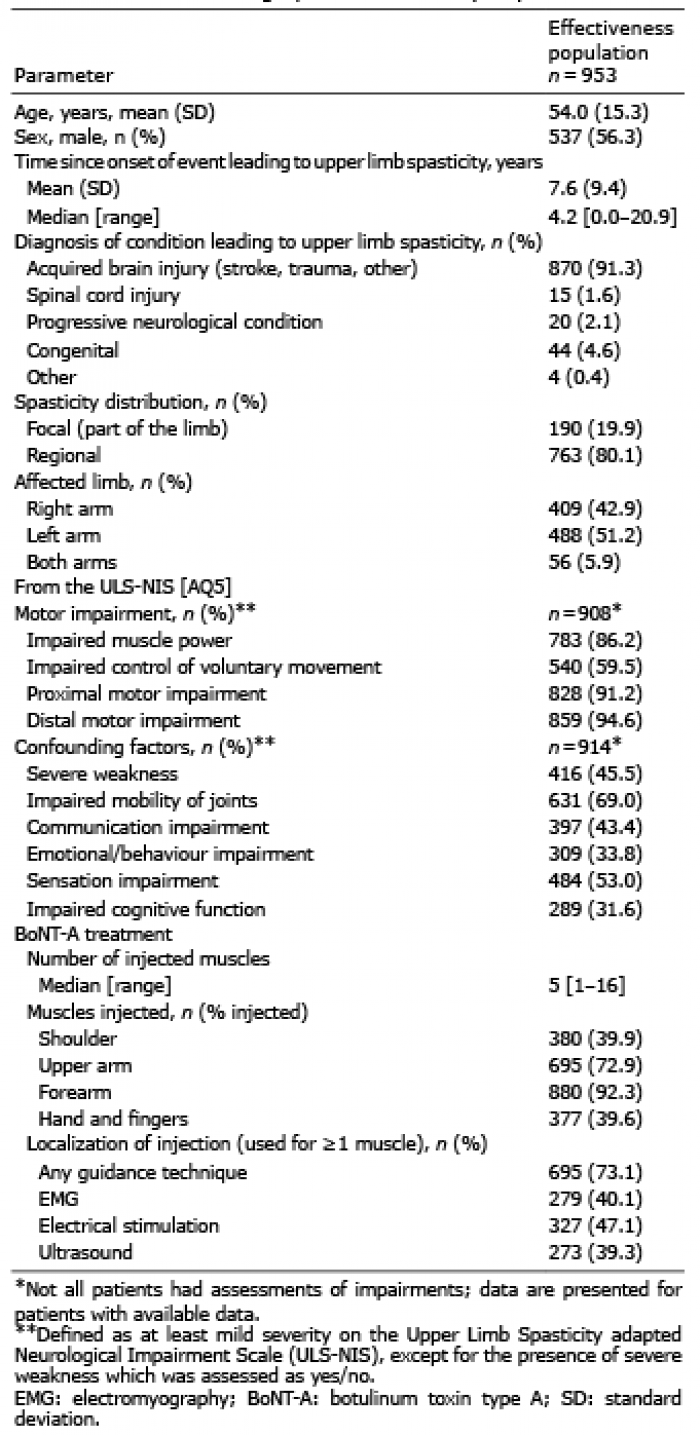 Click to show fullsize
Click to show fullsize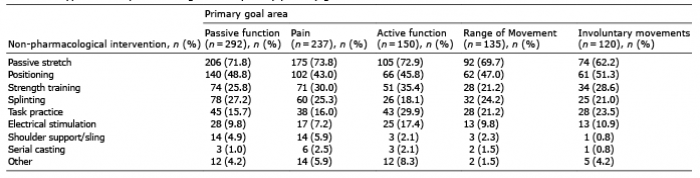 Click to show fullsize
Click to show fullsize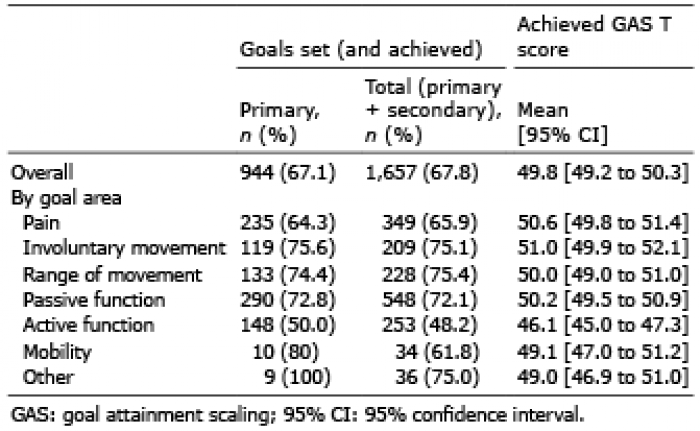 Click to show fullsize
Click to show fullsize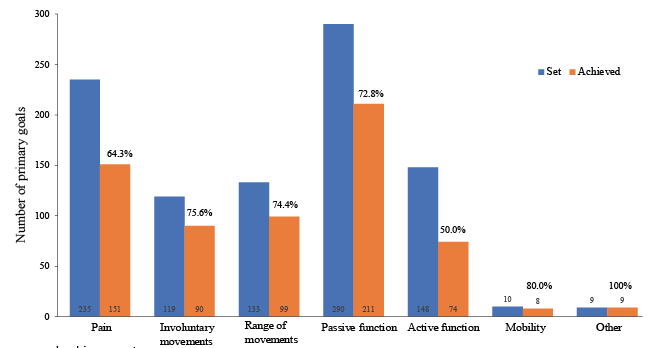 Click to show fullsize
Click to show fullsize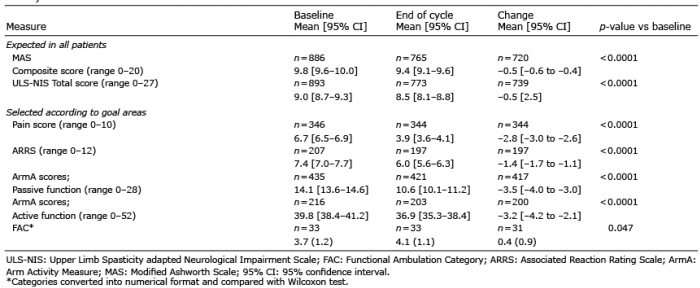 Click to show fullsize
Click to show fullsize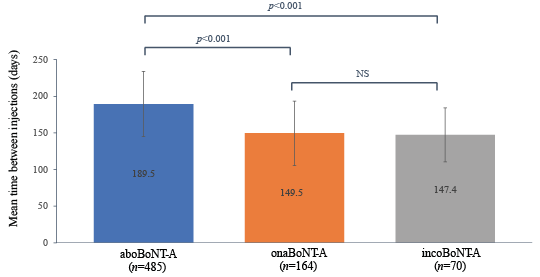 Click to show fullsize
Click to show fullsize